March 7th, 2026
 Latest research studies show why it is critical to regularly activate your brain’s unique Glymphatic System–daily!
Latest research studies show why it is critical to regularly activate your brain’s unique Glymphatic System–daily!
See the research below. I’ve highlighted and annotated the essential information for layman’s reading. I’m a bit of a research nerd myself…
As a preview to the research:
This exciting research shows how specific brainwave function, thought to occur primarily only in deep stages of sleep, activates the brain’s highly specialized system that cleanses and removes plaque-producing proteins, the by-product resulting from the brain’s burning of energy every day.
Without a healthy functional Glymphatic System, there is inevitable damage to the brain that leads to various neurodegenerative disease, such as Dementia, Alzheimer’s, Parkinson’s, Lewy Body Disease and other related neurological disorders.
The research below investigates the importance of the Glymphatic System and how it is activated, as well as what impedes its function.
 This information also helps us to realize the significance of why and how the Healing Spectrums Method can be a highly valuable adjunct not only for regular activation of this powerful brain-cleansing system (even outside of sleep stages), but also how it can cultivate and maintain greater, lasting functionality of this all-important life-supporting system.
This information also helps us to realize the significance of why and how the Healing Spectrums Method can be a highly valuable adjunct not only for regular activation of this powerful brain-cleansing system (even outside of sleep stages), but also how it can cultivate and maintain greater, lasting functionality of this all-important life-supporting system.
So here we go! Note: My annotations are in parentheses and italicised in this blue color. They are not part of the original document and are only my comments to help simplify.
Potential Restorative Function of the Glymphatic System
Natalie L.Hauglund13ChiaraPavan13MaikenNedergaard12
Original Document Link and References:
https://doi.org/10.1016/j.cophys.2019.10.020
Sleep is vital and universal across all species studied, and lack of sleep has detrimental consequences for the organism. (Impacting both physical and emotional health and well-being.)
A broadly accepted theory for the purpose of sleep has yet to be defined. The discovery that sleep, but not wakefulness, allows removal of waste metabolites from the brain defines a new and interesting hypothesis for explaining the biological necessity for sleep: Sleep is for clearing the brain from the potential neurotoxic waste products that accumulate during wakefulness. Brain waste removal is driven by cerebrospinal fluid transport. We have denoted this pathway the ‘glymphatic system’ (You can think of the Glymphatic system much like your car’s catalytic convertor, which helps to remove some of the corrosive hydrocarbons produced by the burning of energy (fuel). Over time, if that system fails, there can be an accelerated rate of corrosive buildup in the engine. There will be a more rapid decline in optimal performance and efficient function, resulting in more visits to you friendly mechanic! It would also result in a shorter life-span of the vehicle.) due to its functional resemblance with the lymphatic system in peripheral tissues and due to its dependence on glia. We here review recent developments focusing on the glymphatic system and sleep and suggest future studies that could shed new light on the reasons for the necessity of sleep for brain health.
Introduction
Sleep is a biological state bringing great vulnerability to the organism, but having a necessary function for health and well-being [1] that has long baffled scientists. The sleep state is characterized by reduced environmental awareness and hinders the execution of other vital behaviors such as feeding or vigilance against predators, which underscores the premise that sleep must subserve fundamental biological benefits. Emerging evidence shows that sleep serves a pivotal function in removal of metabolic waste products from the central nervous system (CNS) via the glymphatic system. (Amyloid-β (Aβ) is a metabolic by-product whose aggregation into amyloid plaques is implicated in neurodegenerative processes such as Alzheimers, dementia, Parkinson’s, etc.)
The glymphatic system denotes the perivascular pathways whereby cerebrospinal fluid (CSF) enters the brain parenchyma, mixes with interstitial fluid (ISF), and then exits the brain via venous drainage [2]. Glymphatic activity is low during wakefulness but active in natural sleep (A high amplitude of the Delta brainwave frequency, normally only occurring at key moments of deep sleep, is necessary for activation of the Glymphatic System. On the other hand, a high degree of the much faster Beta (BW) brainwave frequency is necessary during the waking state. (Beta BW helps us in thinking, processing information, communication, analysis, problem solving—in general, stuff we do in our everyday lives when we are not sleeping.) or under certain types of anaesthesia [3••,4••], suggesting that cleaning of the brain is one of the reasons for the necessity of sleep.
Although several research groups have challenged the concept of a glymphatic system [5, 6, 7], an increasing body of literature supports its existence and increases our understanding of its regulation, functions, and implications. Indeed, impaired glymphatic function has been linked to old age [8] and Alzheimer’s disease (AD) [9], (Other research has indicated that by the age 40-45 the brain generally begins losing the ability to produce Delta BW, thus further diminishing it’s ability to activate the important Glymphatic cleansing system. The good news is…that scientific studies have shown the Healing Spectrums Method and Coherence Activations enliven this important, natural “healing” brainwave. See more here: https://thomasgates.com/archives/7118) and several lines of evidence suggest a highly complicated relationship between glymphatic clearance, sleep, amyloid-β (Aβ), and the water channel AQP4. This review will present results of recent efforts to resolve the relationship between sleep and the glymphatic system and explain the health consequences of poor sleep for brain clearance. Further, we will review emerging evidence that factors linked to glymphatic function might directly affect sleep quality.
The glymphatic system
Removal of waste products from the brain is conducted by cerebrospinal (CSF) (CFS is like the detergent working in your dishwasher. But then…(next highlighted note) that is produced by the choroid plexus within the ventricles. Driven by a pressure gradient, CSF moves along the subarachnoid space between the meninges and the cortical surface. From the brain surface, CSF moves deeper into the cortex via the periarterial space — a fluid-filled gap surrounding penetrating arteries – and then enters the brain parenchyma through aquaporin-4 (AQP4) water channels, which are expressed on the end feet of astrocytes surrounding the periarterial space [2]. Once in the brain parenchyma, CSF mixes with ISF, which contains metabolic waste products released from neurons and non-neuronal cells of the brain. (CSF (cerebral spinal fluid) is like the detergent running through the dishwasher. ISF (interstitial fluid) is like the mix that now has the loose stuff you want to be rinsed away. The rinse cycle can now wash away the waste collected and send it out through the drain (perivenous space). Voila! Clean dishes /brain).
The CSF/ISF mixture exits the brain via the perivenous space as well as cranial nerves and drains to the periphery, carrying with it a sampling of the interstitial contents. Thus, the glymphatic system is a highly organized fluid transport system, which facilitates the clearance of waste metabolites such as tau protein [10], amyloid-β [2] and lactate [11] from the brain.
The glymphatic system and sleep
The relationship between glymphatic flux and sleep was first described by Xie et al., who compared brain influx of CSF tracers in awake, asleep, or anesthetized mice [3••]. In awake mice, hardly any tracer entered the brain, but almost immediately after onset of sleep or induction of anaesthesia, significant tracer influx occurred.
Furthermore, sleep and anaesthesia were associated with a volume increase of the brain extracellular space, which the authors suggested might reduce the resistance to fluid flow and thereby be responsible for the ‘activation’ of the glymphatic pathway during sleep or anaesthesia. The difference in CSF distribution between wakefulness and anaesthesia is supported by results from Ma and colleagues who showed that tracer injected into the CSF of awake mice rapidly reached lymphatic vessels in the periphery, while the tracer in anaesthetized mice instead was transported to the paravascular spaces of the brain [12].
The glymphatic system’s dependence on sleep and anaesthesia has been challenged, for example, by Gakuba et al., who reported no difference in glymphatic influx in mice anaesthetized with isoflurane and ketamine versus awake, post-anesthetized mice [7]. This discrepancy might be explained by recent work by Hablitz et al. who showed that CSF tracer influx is not regulated by wakefulness versus unconsciousness, but rather depends on the magnitude of slow wave activity (SWA) [4••]. Slow waves or delta waves are high amplitude 0.5–4 Hz brain waves that characterize the electroencephalographic (EEG) signal of deep sleep (These slow frequency/high amplitude Delta waves, normally found in stages of deep sleep, are the same Delta brainwaves seen during the Healing Spectrums Sessions initial research studies. The significant difference is that this specific Delta BW will be present for only about 25% of an 8 hour period of sleep. During the Healing Spectrums brainwave studies, the same Delta BW occurred within just a few short minutes of the 10-15 minute Healing Spectrums Session test periods. This is not to say in any way that the Healing Spectrums Sessions can replace the multiple benefits of regular deep sleep. It can serve as an effective adjunct to improve the quality of sleep and lead to easier activation of the Glymphatic System.)
and certain types of anaesthesia, and are considered an indicator of sleep pressure [13]. By analyzing glymphatic tracer influx under different anaesthesia regimens, Hablitz et al. showed that anaesthetics associated with high SWA, such as the alpha-2 adrenergic receptor agonists xylazine and dexmedetomidine, increased glymphatic influx, while anaesthetics associated with low delta power, such as isoflurane, potently suppresses influx.
These findings are supported by other studies reporting the facilitating effect of dexmedetomidine on glymphatic influx [14,15]. Thus, the unchanging glymphatic activity reported by Gakuba et al. likely resulted from their use of isoflurane anaesthesia before tracer injections. Furthermore, the acute post-anaesthetic state differs fundamentally from the awake state, being characterized by confusion, reduced consciousness, and in some cases delirium [16]. Thus, the ‘awake’ mice of Gakuba et al. were likely still in a physiologically impaired condition after having undergone anesthesia and surgery 60 min before the tracer experiment.
While SWA apparently facilitates glymphatic function, the neuromodulator norepinephrine (NE) has a suppressive effect [3••]. NE promotes arousal and has regulatory actions both on neuronal and non-neuronal cells. Specifically, the transition from sleep to wakefulness is associated with increased interstitial NE levels, whereas NE inhibition promotes sleep [17]. The dependence of glymphatic influx on low noradrenergic tone and high SWA presents interventions to promote brain-wide drug distribution.
Thus, Lilius et al. found that intrathecal delivery of small-molecular weight drugs into the brain was improved when co-administered with dexmedetomidine, an adrenergic drug that induces a sedated state with increased slow-wave power and decreased noradrenergic tone [14].
In conclusion, high SWA supports glymphatic activity, but NE signaling in brain (such as occurs during wakefulness) has an attenuating effect. (Deep sleep—more glymphatic function. Wakefulness—not so much…)
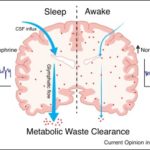
Thus, nREM sleep and certain types of anaesthesia, such as xylazine and dexmedetomidine, enhance glymphatic clearance, while wakefulness, isoflurane and so on, antagonize it (Figure 1).
Download full image
Figure 1. The relationship between glymphatic system function and brain states. In non-rapid eye movement (nREM) sleep or anesthesia-induced states of high delta power and low norepinephrine (NE) tone (left), CSF enters the brain parenchyma, interchanges with interstitial fluid and clears the brain of waste metabolites. In wakefulness or under certain anesthesia that induce a wake-like electroencephalographic (EEG) pattern, and in pharmacologically induced states of high NE tone (right), glymphatic CSF influx decreases, and clearance of metabolic waste products from the brain is attenuated.
Sleep, glymphatic clearance, and amyloid-β
Amyloid-β (Aβ) is a metabolic by-product whose aggregation into amyloid plaques is implicated in neurodegenerative processes [18]. (Deep sleep or additional ways to activate necessary BWA… As long as it happens! )Aβ is removed via the glymphatic pathway [2] and, as discussed above, deep sleep is a prerequisite for glymphatic activity. After sleep deprivation, both animals and humans exhibit increased levels of Aβ in the brain [19••,20]. In fact, disrupting the slow waves of deep sleep is enough to abolish waste clearance [21•].
A gradual brain accumulation of Aβ plaques is one of the hallmarks of Alzheimer’s disease (AD), and poor sleep quality is an independent risk factor for developing AD [22,23]. (Thus, the importance of a good night’s sleep!. However, if there is a diminished capacity for the brain to proceed adequate Delta BW, as happens as we age beginning around the age of 40-45, then the quality and time of Glymphatic System function will be reduced. Healing Spectrums has been shown to help activate higher Delta BW, even in older subjects.) Recently, Winer et al., showed that lower amplitude of slow waves <1 Hz predicted higher Aβ brain levels in patients, while impaired coupling between slow waves and sleep spindles — short bursts of neuronal activity occurring in nREM sleep — predicted greater Tau burden [24].
Between 25 and 60% of patients with AD present with dysfunctional sleep [25], but the association between AD and sleep is bidirectional: not only does dysfunctional sleep contribute to the AD phenotype, but Aβ deposition itself leads to sleep disturbances [26]. Individuals with early increases of Aβ in the CSF but intact cognitive function show increased wakefulness and worse sleep quality, and higher brain Aβ burden is associated with longer sleep latency (time to fall asleep) [27].
Also experimentally this association has been established; in fruit flies, significant sleep fragmentation was reported in flies expressing the human Aβ42 transgene in neurons [28], and in another fruit fly study, sleep medication was sufficient to reverse AD-associated cognitive impairment [29]. Furthermore, sleep disturbances in a transgenic mouse model of Aβ build-up was reported to be rescued if the Aβ aggregation was eliminated [30].
Impaired glymphatic clearance leads to increased Aβ levels in the brain interstitium [2]. Interestingly, the presence of Aβ in the brain can itself impair glymphatic function [9], implying a feed-forward pathway where initial amyloid aggregation is amplified. As such, finding a way to boost glymphatic efficiency could have important clinical implications. (Healing Spectrums enliven the same brainwave function required for activation of the glymphatic System. Yet there can be a simultaneous state of restful alertness (Alpha BW). Not usually the case only during deep sleep.)
Exciting new studies show that increasing the density of meningeal lymphatic vasculature by treating transgenic mouse models of AD with vascular endothelial growth factor boosts glymphatic clearance and decreases brain Aβ levels [31,32]. Another study showed that inhibiting the wake promoting neuromodulator orexin could decrease brain Aβ in mice [20]. Thus, although no clinically translatable pharmacological therapies for boosting glymphatic clearance so far exist, there is sufficient rationale to justify an effort in this direction. (Healing Spectrums enliven the same brainwave function required for activation of the glymphatic System. Drug free…)
Aquaporin-4 in sleep and glymphatic function
AQP4 water channels subserve fast and efficient CSF transport from the perivascular space into the ISF compartment, and loss of AQP4 polarization, which refers to expression localized to astrocytic vasculature-wrapping end-feet, reduces glymphatic clearance [8,9,33, 34, 35]. However, recent findings indicate that AQP4 is not only important for brain waste removal via glymphatic activity, but directly affects sleep architecture.
From analyzing a cohort of cognitively normal old adults, Rainey-Smith et al. found that genetic variants in human AQP4 directly modified sleep quality [36••], a finding that may help explain the large genetic contribution to the inter-individual variation of the sleep EEG [37]. Interestingly, the relationship between AQP4 and sleep appears to be reciprocal, as mice deprived of sleep for 48 hours loose AQP4 polarization [38].
Because AQP4 function has implications for intracerebral Aβ accumulation, and given that Aβ can itself alter sleep patterns, it is difficult to determine whether AQP4 alone is able to moderate sleep quality, or if impaired metabolic waste clearance is a contributing factor (Figure 2). A study looking specifically at AQP4 in relation to Aβ clearance showed that AQP4 knockout mice had impaired Aβ clearance from brain and CSF [2], and that AQP4 deficiency exacerbates brain Aβ plaque deposition in APP/PS1 mice (a mouse model of AD) [39].
Similarly, post mortem examination of human AD patients shows abnormal AQP4 expression with enhanced AQP4 immunoreactivity around Aβ plaques [40]. These observations would support the clinical use of AQP4-targeting therapeutics against AD, but unfortunately no appropriate AQP4-specific drugs have yet been identified [41]. Future research should focus on pharmacologically modulating AQP4 function, polarization and expression, which could elucidate the mechanisms linking sleep, AQP4 and glymphatic function, and possibly introduce new lines of treatment.

Download full image
Figure 2. The multi-directional interrelation between sleep, aquaporin-4 (AQP4), amyloid-β accumulation, and glymphatic clearance. While genetic variations of aquaporin-4 (AQP4) can alter sleep quality [36••], poor sleep quality induces AQP4 depolarization (defined as loss of localized AQP4 expression in vasculature-wrapping astrocytic end-feet) [38], which in turn impairs glymphatic clearance [8,34,51] and induces amyloid-β (Aβ) accumulation [2,39,40].
The glymphatic system prevents Aβ accumulation [2], (Properly functioning Glymphatic System serves as a preventative for Alzheimer’s and other neurodegenerative diseases such as dementia, Parkinson’s, ALS, etc.) which in itself can directly decrease glymphatic influx [9] and impair sleep quality [27,30,50], which independently suppresses glymphatic clearance [3••]. Red lines indicate a negative impact and black lines indicate a positive impact. Dotted lines indicate associations that may be downstream results of impaired glymphatic clearance and/or Aβ accumulation. The parentheses around [3••] indicates that this study did not directly test the impact of poor sleep quality on glymphatic clearance, but showed that sleep activates glymphatic clearance. (But disruptive sleep patterns can interfere with the enlivenment of the necessary specific brainwave activity. Again, approximately only 25% of an 8 hour period of sleep, on a good night. If sleep cycles are interrupted at key moments, then sleep may not always produce the desired effects of Glymphatic cleansing.) The parenthesis around [39] indicates that this study did not directly test the impact of AQP4 polarization on Aβ accumulation but showed that the deletion of AQP4 exacerbates cognitive deficits and progressive Aβ accumulation in APP/PS1 mice.
Unanswered questions
The novel concept that one of the functions of sleep is to clear metabolic waste from the CNS has motivated research efforts focused on understanding the mechanisms by which glymphatic clearance and sleep are interconnected. However, several crucial questions remain to be answered. Importantly, the mechanism that inhibits CSF influx to the brain during wakefulness but promotes its entry during sleep is not yet characterized.
The increased extracellular space volume (Research has shown that our brains actually shrink during sleep. (Don’t worry, it’s a good thing!) This brain reset, known as “synaptic homeostasis,” allows the brain’s synapses, or the connections among neurons, to shrink by nearly 20%. This process has a two-fold purpose:
1. It prevents the synapses from becoming overloaded and burned out after the day’s activities and allows the brain and body to refresh and recharge.
2. The brain’s reduced volume then enhances the effective flow of CSF and IST during the Glymphatic System function, thus providing the important rinsing away of the damaging waste proteins that contribute to various neurodegenerative diseases. It’s your brain’s own version of a catalytic converter.)
associated with sleep is at least in part responsible [3••], but the molecular mechanisms driving a rapid change in the extracellular volume fraction remains to be defined.
The finding that glymphatic influx correlates with the amplitude of SWA [4••] points to an interesting connection between the glymphatic system and sleep homeostasis. Sleep pressure, the subjective sense of urgency for sleep after extended wakefulness, correlates with increased delta power in the EEG, while recovery sleep normalizes the elevated delta power [42, 43, 44]. Thus, it would be expected that glymphatic activity might be highest during the first part of the sleep period, where sleep pressure/delta power is highest.
Further issues are whether increased sleep pressure in wakefulness has the ability to increase glymphatic influx despite the fact that wakefulness normally shuts down glymphatic clearance, and if local sleep, or local occurrences of delta power in the awake brain [45], can locally increase fluid fluxes. (Beta BW, the most predominate brainwave functioning during general wakefulness, is on the opposite end of the spectrums from Delta BW. So it stands to reason that wakefulness would shut down the Glymphatic System. But would it be possible to have some state of wakefulness simultaneously with the Delta BW? This is possible when in a state of “restful alertness.” We have seen high levels of Alpha along with hi levels of Delta simultaneously during the Healing Spectrums brainwave studies. More on this: https://thomasgates.com/archives/6531)
So far, no studies have investigated if glymphatic clearance occurs during REM sleep, but a possible hint comes from a recent functional ultrasound imaging study reporting that REM sleep is associated with a brain-wide increase in cerebral blood volume [46]. Such hyperemic events could well alter CSF influx, as arterial pulsation has already been shown to be an important driver of CSF flow [47, 48, 49]. Other physiological changes that occur in the transition from nREM sleep to REM sleep, such as the decrease in NE tone and delta power and the increase in heart rate, also likely impact glymphatic activity, but future studies are needed to elucidate the relationship between sleep phase and glymphatic clearance.
Most studies to date have focused on glymphatic activity in sleep and anaesthesia. However, it remains a mystery why wakefulness seems incompatible with brain CSF clearance. If waste removal from the brain is necessary for its health and function, it would seem more intuitive that these clearance processes should work continuously during the wake period to avoid build-up of toxic waste. (See above comment. Essentially, neuronal synapses is necessary for waking state activity such as thinking, analysis, communication, problem solving, visual and auditorial function, etc. You know—the stuff we do during our daytime activities.) We speculate that rapid CSF movement in the brain may simply be incompatible with waking consciousness.
Active glymphatic clearance is associated with larger extracellular space volume combined with active fluid dispersion which will favour glutamate spill-over and thereby promote synchrony of neural activity — a signature of nREM sleep. In other words, the precision in time and space of synaptic transmission, which is a requirement of the awake circuit to process information, may not be compatible with glymphatic fluid transport.
Conclusion
Sleep and anaesthesia-induced states of high delta power drive CSF influx to the brain parenchyma, ultimately washing out waste metabolites via the glymphatic pathway [2,3••,4••]. There is a well-established relationship between sleep, glymphatic clearance and Aβ washout, although complicated by their bidirectional links [27,30,50]. Furthermore, AQP4 depolarization on astrocytes is linked both to glymphatic clearance and sleep [2,36••]. So far, most studies of the glymphatic system have focused on establishing how pathological conditions or different anaesthesia regimens affects glymphatic clearance. However, the basic mechanisms driving CSF flow during sleep remain to be elucidated. So far, we have not fully plumbed the depths of this highly dynamic fluid transport system, which is critically controlled by diverse factors such as brain state, the cardiovascular system, plasma osmolarity, and is implicated in neurodegenerative disease.
Current Opinion in Physiology 2020, 15:1–6
This review comes from a themed issue on Physiology of sleep
Edited by A Jennifer Morton and Vladyslav Vyazovskiy
https://doi.org/10.1016/j.cophys.2019.10.020
2468-8673/© 2019 Elsevier Ltd. All rights reserved.
© 2019 Elsevier Ltd. All rights reserved.
Filed under Blog | Comments Off on Turn on Your Brain’s Powerful Rinse Cycle! Maintaining Healthy Brain Function

 There are many posts here covering a wide range of topics from NDEs to Death, Grief & Spirituality, Angels, Consciousness, Alternative Health, Brainwave Studies, Self-Healing, and more!
There are many posts here covering a wide range of topics from NDEs to Death, Grief & Spirituality, Angels, Consciousness, Alternative Health, Brainwave Studies, Self-Healing, and more!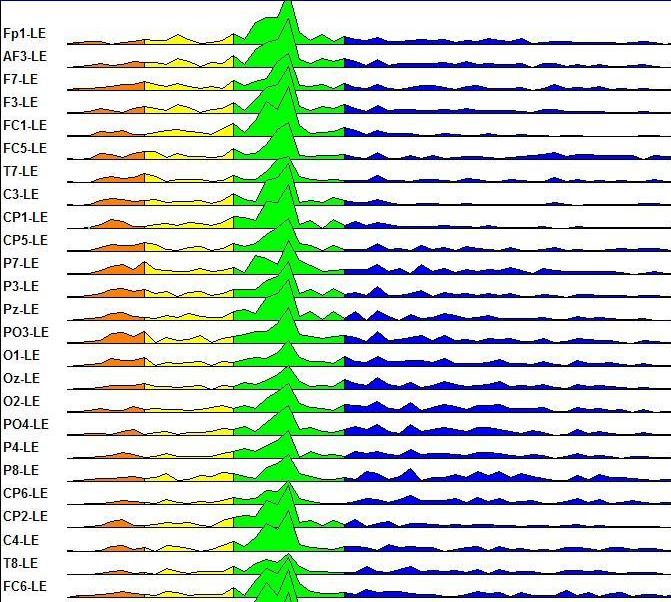


{kind=link}
{kind=link}